Hypoplastic Left Heart Syndrome (HLHS)
Copyright 2007
Definition
Hypoplastic left heart syndrome is the incomplete formation of the chambers, valves, and or vessels of the left side of the heart. Infants with HLHS are also born with additional defects including ventricular septal defect, patent ductus arteriosus, and narrowing other parts of the aorta.
During development blood flow is needed to enable the structures of the cardiovascular system to fully develop. If blood flow through a particular structure is decreased due to a congenital abnormality, then not only does it develop poorly, but all the structures downstream develop poorly. Thus if there is congenital mitral stenosis or mitral regurgitation, then associated hypoplasia of the left ventricle, aortic valve and aorta results. Similarly on the right side of the heart. If there is tricuspid stenosis or tricuspid atreasia or even Ebstein’s anaomaly, flow is decreased resulting in a myriad of hypoplastic events downstream and hence the hypoplastic right heart sysndrome. There are varying severities and degree of involvement in each of these syndromes – sometimes incompatinble with life, sometimes amenable to surgery and sometimes mild enough not to be even detected.
With poor systemic supply of oxygenated blood from the left heart, the ductus arteriosus usually remains open so that blood, albeit deoxygenated blood from the pulmonary circulation, is able to provide some blood to the systemic circulation. Mixing of deoxygenated and oxygenated blood therefore occurs. Infants are born with extremely low oxygen saturation rates as well as respiratory distress. HLHS can be fatal within hours if untreated. Standard fetal ultrasound is used to diagnose HLHS. This defect is not entirely curable. Various surgical treatments exist in stages including cardiac transplantation if HLHS is severe. The Norwood procedure is commonly performed as the first stage followed by a second procedure which establishes adequate connection for the systemic and and pulmonary circulations.
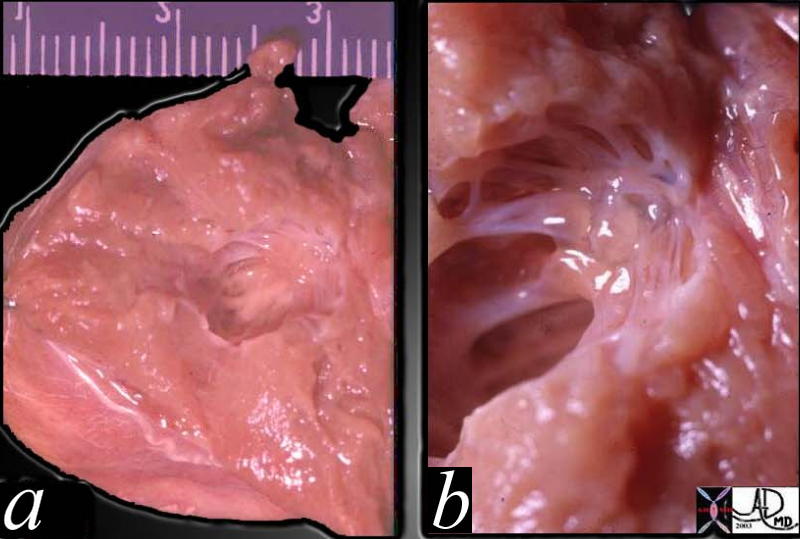
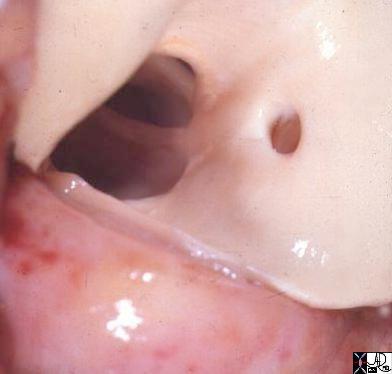
This pathological specimen is from a patient with hypoplastic left heart syndrome, (HLHS) (a) show a diminutive LV cavity (about 5mm in diameter)and MV elements with a relatively thick LV wall. (about 9mms in diameter) Both these findings are characteristic of the disease. a close-up of the MV (b)shows an atretic MV with unformed and poorly formed elements including the chordae and papillary muscles. No lumen could be identified.
Courtesy Ashley Davidoff MD. TheCommonVein.net 01813c01
keywords heart cardiac congenital gross pathology HLHS MV cavity LV wall mitral atresia
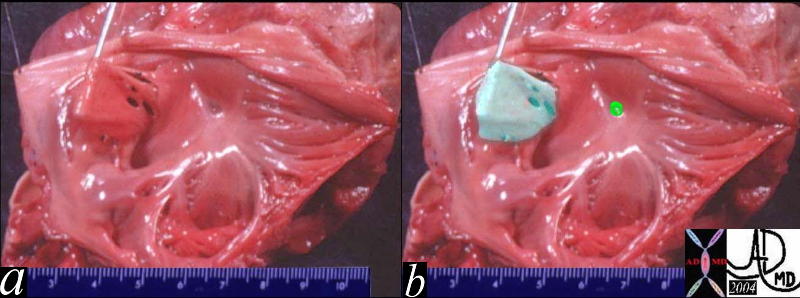
This is a pathologic specimen of a patient with mitral valve atresia (lime green overlay in b) in this view of the left atrium. The atrial septum shows a redundant perforated septum primum that was restrictive to the high pressure in the LA and an aneurysm resulted. (pale green overlay in b)
Courtesy Ashley Davidoff MD. TheCommonVein.net 06829c02
key words CVS cardiac heart MV atrial septum ASD aneurysm mitral atresia LA congenital gross pathology
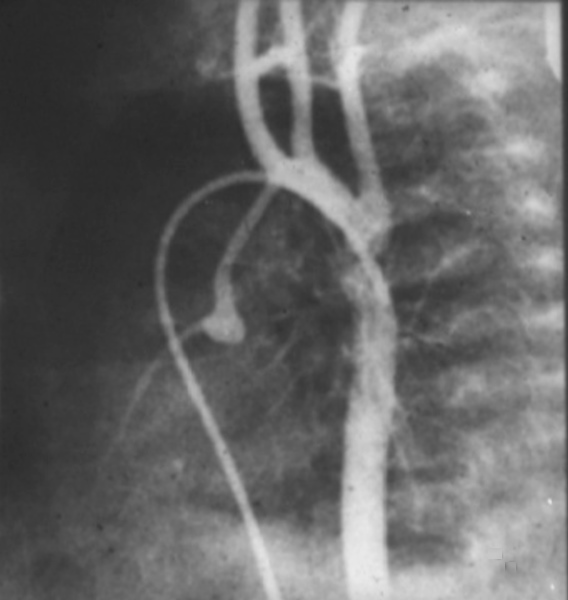
The catheter for tis angiogram was advanced from the femoral vein into the RA then to RV and then via a PDA into the aorta. Contrast injected into the descending aorta flowed retrograde into the ascending aorta since this was of low pressure die to the atretic aortic valve not being in communication with the systemic pressure of the LV. The coronaries are also filled in retrograde fashion. The ascending aorta is severely narrowed, the arch is hypoplastic and there is a coarctation. This is only part of the hypoplasia of the left system which more often than noot involves varying degrees of atresia and hypoplasia of the LV and mitral apparatus.
keywords heart cardiac coronary artery aorta small dx aortic atresia tubular hypoplasia aortic coarctation aortic atresia PDA patent ductus arteriosus angiogram angiography CHD congenital heart disease Ashley Davidoff MD TheCommonVein.net 00269b02
Ashley Davidoff MD TheCommonVein.net 15049
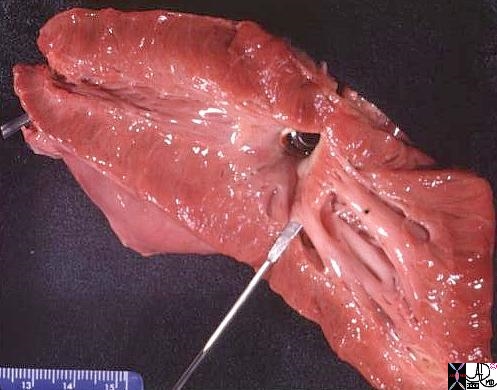
The anatomical specimen is from a patient with mild hypoplastic left heart syndrome requiring aortic valve replacement. There was only mild mitral valve disease but there was significant aortic stenosis requiring valve replacement. The chordae in this case are thickened and foreshortened though the papillary muscles are well developed.
keywords heart LV left ventricle mitral valve MS AS aortic valve stenosis HLHS hypoplastic left heart syndrome gross pathology
Courtesy Ashley Davidoff thecommonvein.net 01818.6s
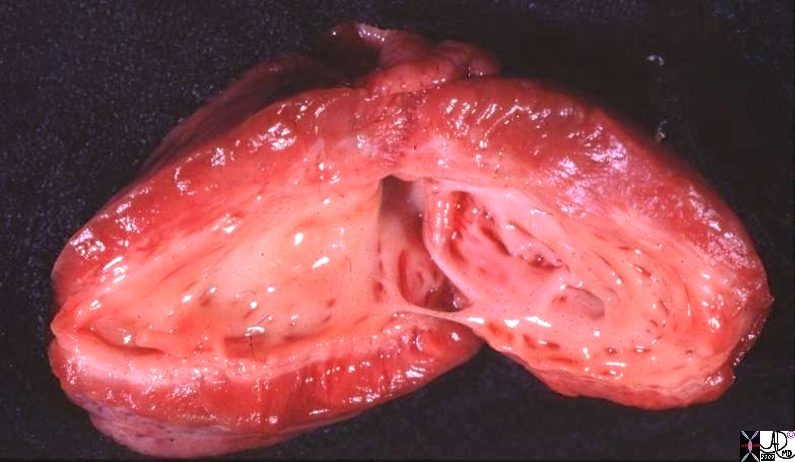
The gross pathology specimen is a case of hypoplastic left heart with aortic stenosis and mitral stenosis, revealing a thickened endocardium with left ventricular hypertrophy, deformed and thickened mitral valve and papillary muscles. The thickened endocardium is caused by the high pressures generated in the LV causing subendocardial ischemia and a resulting in a condition called endocardial fibroelastosis. (EFE)
Courtesy Ashley Davidoff thecommonvein.net 08058.8s
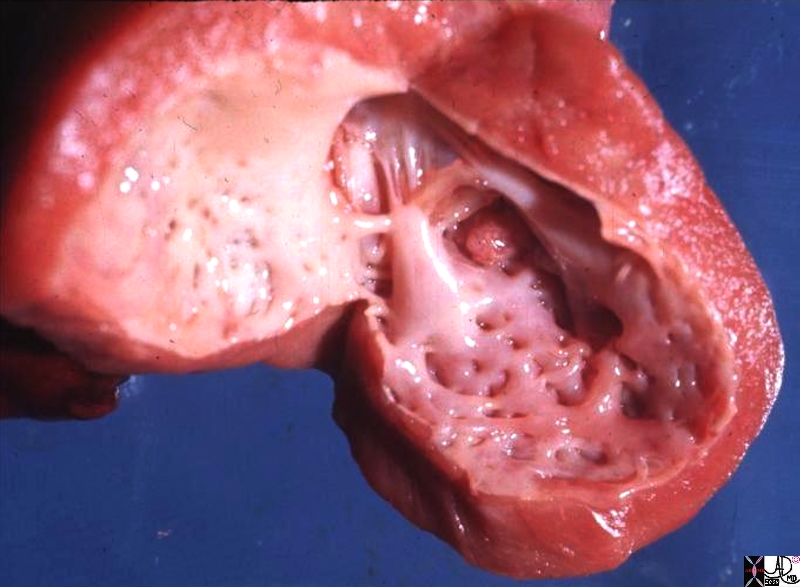
Second Case of EFE
The gross pathology specimen is a case of hypoplastic left heart with aortic stenosis and mitral stenosis, revealing a thickened endocardium with left ventricular hypertrophy, deformed and thickened mitral valve and papillary muscles. The thickened endocardium is caused by the high pressures generated in the LV causing subendocardial ischemia and resulting in a condition called endocardial fibroelastosis. (EFE) heart cardiac gross pathology
Courtesy Ashley Davidoff Copyright 2009 08061b.8s