PARTS
Copyright 2007
Introduction
Ashley Davidoff
The aorta is divided in general into the thoracic aorta and the abdominal aorta. The thoracic aorta start at the level of the aortic valve, and continues as the ascending portion, the arch and the descending portion. The main divisions of the abdominal aorta are the suprarenal and infrarenal portions, which are demarcated by the departure of the renal arteries from the aorta around the top of the second lumbar vertebra. This breakdown is commonly used by vascular surgeons when characterizing the locations of abdominal aortic aneurysms.
Thoracic Aorta
Parts of the Thoracic Aorta |
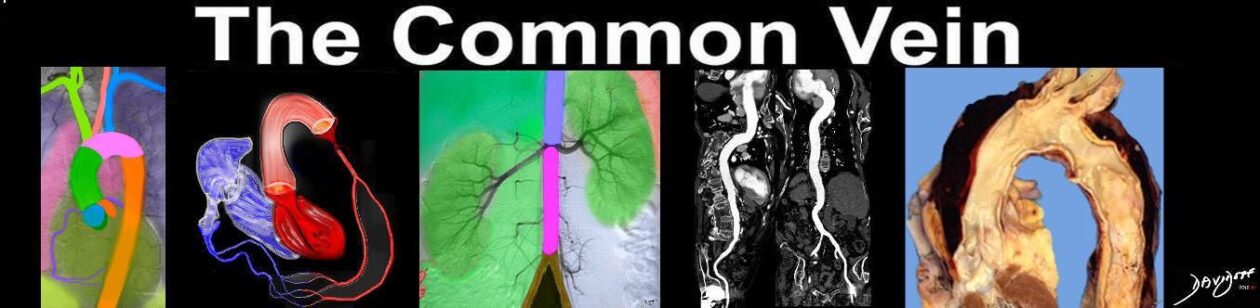
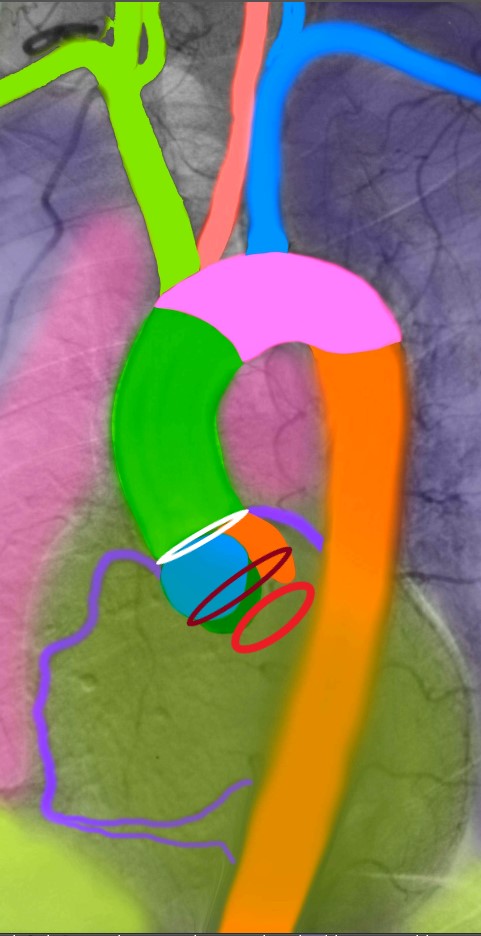
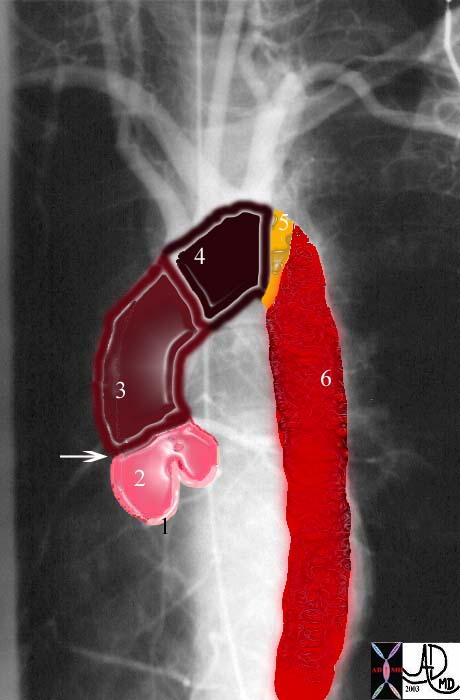
| This is an angiogram of the aorta in LAO projection showing the component parts of the thoracic aorta. The pink aortic valves (1) lie between the L and the sinus or bulbous portion of the aorta. (2) The tubular portion of the ascending aorta extends for about 5cms, from the sino tubular junction (arrow) to the origin of the brachiocephalic artery. (3) The aortic arch (4) extends to the level of the isthmus, (5) which is at the level of the insertion of the ligamentum arteriosum. The descending thoracic aorta (6) courses alongside the vertebral body to reach the aortic hiatus.
Courtesy Ashley Davidoff MD. 27185g code aorta CVS normal thorax parts |
Annulus
The aortic annulus is the ringed juncture of the outer wall of the aortic valve and ascending aorta. It is characterized structurally by its circular geometry, approximately 3-3.7 cm in diameter. It acts as the foundation for the attachment of the aortic valve. Common diseases include calcified aortic sclerosis and syphilitic aortitis. As a distinct structure it is not easily appreciated by conventional imaging but when calcified for example in aortic sclerosis, it is easily seen by CTscanning. In the case of a ring abscess caused by bacterial endocarditis this entity is well seen by echocardiography. Treatment of this structure is surgical.
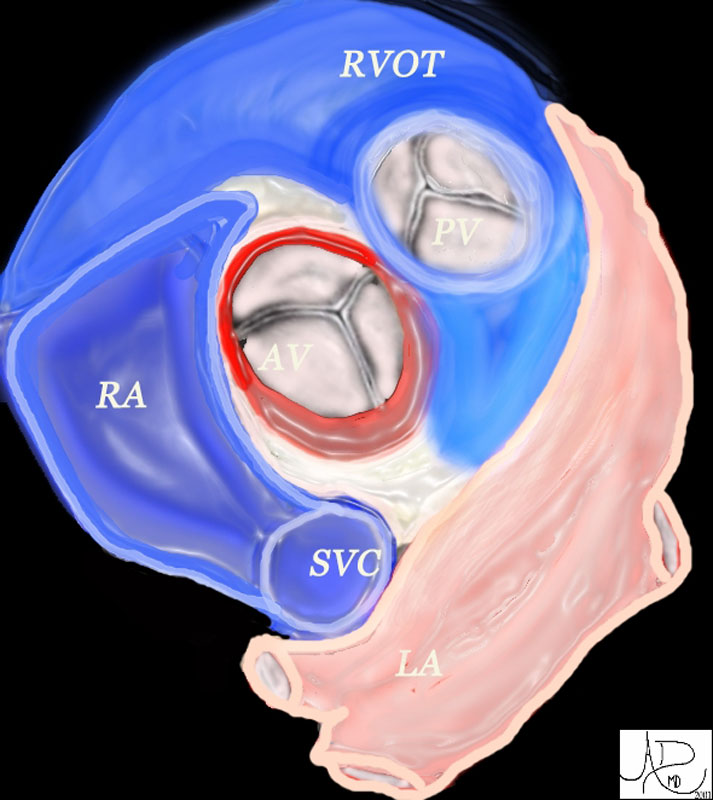
The aortic valve (AV) lies central to many structures including the right ventricular outflow tract (RVOT), pulmonary valve (PV), left atrium (LA), right atrium (RA), and superior vena cava (SVC). aorta from above. In this diagram, the commissures are overlaid in green, the crescent shaped lunulae reflect the free edge of the leaflets and are overlaid in yellow, and the nodules of Arantii are overlaid in orange. The sinuses of Valsalva are like cups and are positioned between the free edges. (gray)
Davidoff art Ashley Davidoff MD TheCommonVein.net 47681Aortic Valve
The aortic valve is one of the four valves of the heart, located between the left ventricle and the base of the aorta. It is characterized structurally by three leaflets in a semi lunar shape. In the middle of each leaflet is a small bulge or nodule called Arantius’ nodule. The root of the valve is attached to the aorta in a curvilinear manner. The one way valve opens passively during systole and closes during diastole. Common diseases include calcific aortic stenosis, aortic regurgitation, bacterial endocarditis which sometimes progresses to ring abscess. Bicuspid aortic valve is one of the most common congenital cardiac abnormalities. Most entities of the aortic valve are best and easily diagnoses by echocardiography. CTscan and MRI are useful as well. Surgical treatment, particularly aortic valve replacement is common, with mechanical prosthetic valves or biological valves. The biological valve is commonly made of porcine valvular tissue, and is called a xenograft. In some cases the valve is harvested from a cadaver and is called a homograft.
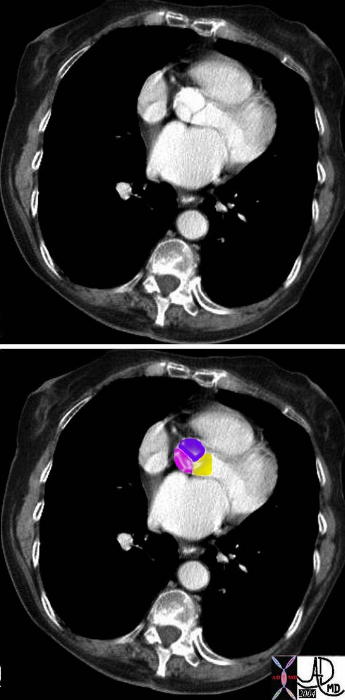
Normal Aortic Valve |
| This image of a CT scan at the base of the aortic valve focuses on the three coronary cusps which are closed in this diastolic phase, revealing the “peace sign” causes by the coapted leaflets. The posterior cusp (pink) is the non coronary cusp, the left coronary cusp (yellow) is in closest contact with the LV outflow tract, and the right coronary cusp, (purple) is the ost anterior. The origin of the right coronary artery can be visualised.
Courtesy Ashley Davidoff MD 38357c01 code cardiac heart aorta RCA sinus of Valsalva imaging radiology CTscan normal anatomy |
Sinuses of Valsalva
The sinuses of Valsalva are dilated cavities between the aortic leaflets and the ascending aortic wall. They are subdivided into the left, right and posterior sinuses. The sinuses are characterized structurally by their bulging shape protruding into the aortic wall. They act as a buffer between the leaflets, giving rise to the left and right coronary arteries at the sinotubular junction. They are not as commonly the source of disease but may rarely become aneurysmal. Sinus of Valsalva aneurysm is most easily diagnosed by echocardiography and requires surgical treatment.

Sinuses of Valsalva and Aortic Valve |
| 35324b03 thoracic aorta ascending aortic valve sinus of Valsalva normal Courtesy of Laura Feldman MD code aorta arch artery ascending descending normal thorax |

Aortic Valve and Sinuses |
| 07970 The aorta and the outflow components of the LV They demonstrate the makeup of the sinus (aka bulbous portion) of the aorta showing the aortic valveand the aortc sinus LVOT has been opened showing the three valve leaflets and their associated sinuses. between the right and non-coronay cusp, while the anterior and posterior branches are distributed in the septum (s). The right and left aortic cusps each contain a coronary ostium The non coronary cusp lies between the the left and right cusps, and is without an ostium. The anterior leaflet of the mitral valve participates as the lateral wall of the LVOT, and is attached to the non and left coronary cusp. Courtesy Ahley Davidoff MD code CVS normal aorta heart LV LVOT left bundle branch mebranous septum sinus of Valsalva left right coronary ostium AO AOV aortic valve commissure imaging radiology anatomy overlay anatomy normal |
Sinotubular Junction
The sinotubular junction marks the boundary between the bulbous portion of the aorta and the ascending proximal aorta. The junction becomes effaced in diseases such as sinotubular ectasia which occurs in MArfan’s disease and syphilitic aortitis which is now rare. Diagnostic studies include echocardiography, CT scan, MRI, and aortography. Treatment is usually surgical.

Sinotubular Junction |
| 35324b06 thoracic aorta ascending normal Courtesy of Laura Feldman MD code aorta arch artery ascending descending normal thorax |
Ascending Aorta
The ascending aorta is the first segment of the aorta’s structural anatomy. It is located between the left ventricle and the aortic arch. The ascending aorta is characterized by its tubular shape and elastic nature. Contained in the pericardium, the ascending aorta runs superiorly, curving obliquely upwards from right to left as it ascends on the right side.. The segment is generally about 5 cm in length. As it commences from the aortic valve, the ascending aorta gives rise to the two coronary arteries which supply the heart. Common diseases include atherosclerosis, aortic aneurysm. When aortic dissection affects the ascending aorta it is an indication for surgery. Diagnostic studies include CT imaging, echocardiography, MRI, aortography, and echocardiography. Treatment in general is surgical.

Ascending Aorta |
| 35324b02 thoracic aorta ascending normal Courtesy of Laura Feldman MD code aorta arch artery ascending descending normal thorax |
Arch
The aortic arch is the segment between the ascending and descending thoracic aorta. Its course begins at the upper level of the second right sternocostal junction. The arch runs upwards in an anterior-superior curve towards the left in front of the trachea. It then proceeds downward passing the left side of the body of the fourth thoracic vertebra and then meets the proximal descending aorta. The aortic arch is characterized structurally by its tubular curvature and elastic properties. At the top of the arch are three arterial branches called as a group the brochiocephalic arteries which carry blood to the head and upper limbs. Common diseases include atherosclerosis and aortic aneurysm. Dissection commonly involves the arch, often originating just beyond the left subclavian artery. Diagnostic studies include CT scanning, aortography, MRI and echocardiography. Treatment is usually surgical.

Arch of the Aorta |
| 35324b01 aorta arch normal Courtesy of Laura Feldman MD code aorta arch artery ascending descending normal thorax |
Isthmus
The isthmus is a slight constriction (approximately 3 mm) of the aorta just proximal to the point of attachment of the ductus arteriosus and distal to the origin of the left subclavian. It is characterized structurally by minimal narrowing of the tubular segment at that point. It serves as a marker for the site of the ductus arteriosus in fetal circulation and for the ligamentum arteriosum, a fibrous remnant in the child and adult. The narrowing of the aorta is simply the remnant of the embryologic structure. Common diseases at this include atherosclerosis, coarctation of the aorta and patent ductus arteriosus. Diagnostic studies include CT imaging, aortography, MRI and echocardiography. Surgical treatment is most common.

Aortic Isthmus |
| 35324b04 thoracic aorta ascending aortic valve sinus of Valsalva normal Courtesy of Laura Feldman MD code aorta arch artery ascending descending normal thorax |
Descending Thoracic Aorta
The descending thoracic aorta is the segment between the arch and abdominal aorta. Within the posterior mediastinal space, the descending thoracic aorta begins at the distal aortic arch at the lower border, and on the left side of the fourth thoracic vertebra. It terminates in line with the lower border of the twelfth thoracic vertebra in front of the diaphragm at the level of the aortic hiatus. The descending thoracic aorta is characterized structurally by its tubular shape and highly elastic composition. As this segment courses downward, it gives rise to the two bronchial arteries as well as most of the posterior intercostals arteries. The artery of Adamkiewicz is a very important small branch that usually arises from one of the left sided posterior intercostals arteries. It supplies the lower two thirds of the spinal cord via the anterior spinal artery.
Common diseases of the descending aorta include atherosclerosis, aneurysmal disease, and aortic dissection. Diagnostic studies include CT imaging, MRI, and aortography. Surgical treatment is most common. Percutaneous placement of endoluminal grafts are evolving as less invasive techniques, but at this stage are more commonly used in the abdominal aorta.
 Descending Thoracic Aorta Descending Thoracic Aorta |
| 35324b05 thoracic aorta ascending aortic valve sinus of Valsalva normal Courtesy of Laura Feldman MD code aorta arch artery ascending descending normal thorax |
Abdominal Aorta
The Abdominal aorta is the last segment of the aorta, commencing at the end of the thoracic aorta and terminating by bifurcation into the common iliac arteries. The abdominal segment originates at the aortic hiatus of the diaphragm at the plane of the thoracic and lumbar vertebral junction. The aorta is surrounded by the right and left crura at this stage. The abdominal aorta is structurally characterized as a tapering tube, composed of muscular and elastic tissue. Along its course, the abdominal aorta gives rise to several large branches including the celiac axis, the superior mesenteric artery (SMA), and the inferior mesenteric artery (IMA arising 3 to 4 cm above the bifurcation. The renal arteries arise from the lateral border of the aorta between the SMA and IMA branches. The gonadal arteries (testicular and ovarian) are small branches that also arise from the lateral border of the abdominal aorta below the origin of the renals and above the IMA. Common diseases include abdominal aortic aneurysm, (AAA – “triple A”) and atherosclerosis. Diagnostic studies include CT imaging, MRI, aortography and ultrasound Treatment is usually surgical, and with percutaneous techniques such as endoluminal graft insertion becoming more frequently utilized.
Suprarenal Abdominal Aorta
The suprarenal aorta as its name implies is that portion of the abdominal aorta that lies above the renal arteries. Its first branch is the celiac axis which arises anteriorly and which itself gives rise to the arteries of the foregut. The superior mesenteric artery arises about 1 cm distally, supplying structures of the midgut. The suprarenal aorta also supplies a number of smaller arteries, including the inferior phrenic arteries, the suprarenal vessels, and the paired gonadal arteries. Atherosclerosis is common in this segment of the aorta but aneurysmal disease is more common in the ingrarenal segment. When aneurysms occur at the level of the renal arteries or above they present a significant challenge for the surgeon.
Ashley Davidoff
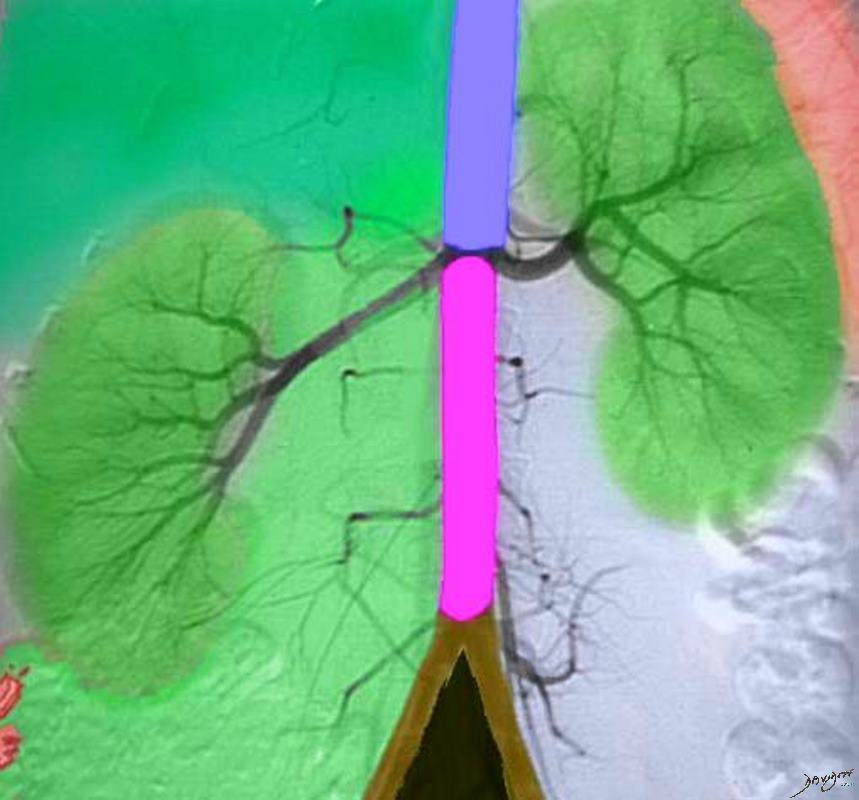
 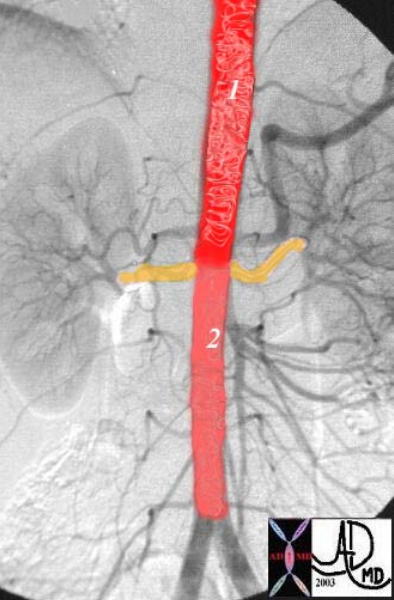 Suprarenal and Infrarenal Abdominal Aorta Suprarenal and Infrarenal Abdominal Aorta |
| This overlay of a normal abdominal angiogram shows the two components of the abdominal aorta. The suprarenal component, (1) is slightly larger than the infrarenal component (2). The renal arteries, (in orange overlay,=) take 20% of the cardiac output and hence a large portion of the aortic blood flow is “unloaded” at this level.
Courtesy Ashley Davidoff MD. 24877d code CVS aorta abdomen normal suprarenal infrarenal |
Infrarenal Abdominal Aorta
The infrarenal aorta as its name implies lies below the origin of the renal arteries. It is located between the top of L2 and the bottom of L4. It gives rise on its anterior surface to the inferior mesenteric artery, supplying structures of the hindgut, and from both posterolateral walls to a number of lumbar vessels, and to a middle sacral artery at the level of the aortic bifurcation. Common diseases include abdominal aortic aneurysm, (AAA – “triple A”) and atherosclerosis. Diagnostic studies include CT imaging, MRI, aortography and ultrasound Treatment is usually surgical, with percutaneous techniques such as endoluminal graft insertion becoming more frequently utilized.