Copyright 2008
Ashley Davidoff MD
Definition
Acute aortic syndrome” (AAS) is a complication of atherosclerotic disease of the aorta that is characterized by a classical clinical presentation of sudden acute searing pain in the chest or back,
Aortic dissection is a sudden catastrophic disruption of the aortic wall caused by a shearing tear of the intima, and secondary involvement of the media by the advancing dissection and hematoma. The event characterized by a splitting of the arterial wall along the longitudinal plane of the aorta.
The pain of aortic dissection is dramatic. It is classically hyperacute, sudden, severe, lancinating, excruciating, tearing, stabbing, throbbing, reaching its maximum intensity at the moment of onset. On the other hand, some patients may present with minimal or no symptoms. The duration of the pain is not measured in minutes and may simulate the pain of myocardial infarction. The pain may be felt in the anterior chest, the neck, and/or the back, sometimes reflecting the location of the dissection with ascending dissections noted with anterior chest pain, arch dissections with neck pain and descending thoracic dissections noted with interscapular or back pain. Since dissections may involve the coronary arteries, and more commonly the right, myocardial ischemic pain may be present as well.
It is historically interesting to note that in 1910 William Osler recognized that “spontaneous tear of the arterial coats is associated with atrocious pain, with symptoms, indeed, in the case of the aorta of angina pectoris and many instances have been mistaken for it”.
The pain is caused by the stretching of the aortic wall, and hence its potential to have a throbbing character. It is not aggravated by position or body movement, nor relieved other than by analgesia, tincture of time, or repair.
The impending sense of doom originally described as “angor animi” literally means anguish of the soul may accompany the pain. This sensation sometimes accompanies other life-threatening situations when there is massive outpouring of catecholamines, such as myocardial infarction and pulmonary embolism.
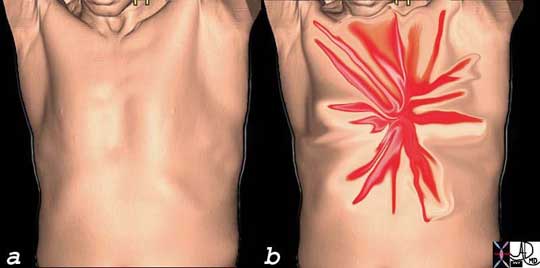
AcuteAorticSyn.jpg
Acute Severe Lancinating, Shearing, Chest Pain of Acute Aortic Syndrome
Ashley Davidoff
The pain of dissection may be felt either in the front of the chest and/or the back. Either way, the pain can have similar characteristics – i.e. sharp, thunderbolt-like, severe, and rapidly and almost instantaneously reaching maximum intensity coincident with the onset.
Courtesy of: Ashley Davidoff, M.D.
usually in the older patient

Ashley Davidoff
TheCommonVein.net
with atherosclerosis
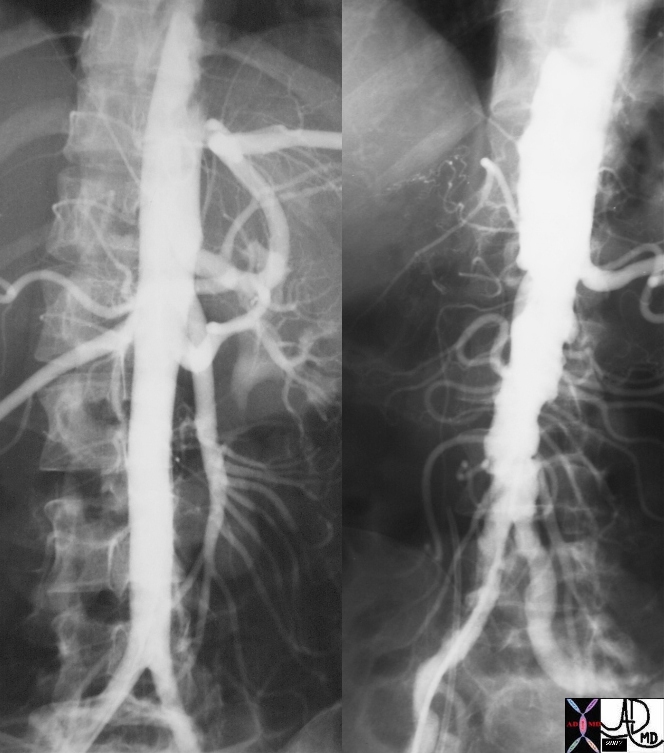
18485c01 aorta artery hepatic artery renal artery splenic artery superior mesenteric artery SMA kidney severe atheroscleroris atheroma occluded renal artery spleen liver normal anatomy angiogram angiography
Ashley Davidoff MD
THECOMMONVEIN.net
usually in an hypertensive patient.
Ashley Davidoff THECOMMONVEIN.net
Copyright 2021
- Life threatening
- high risk of aortic rupture and sudden death
- aortic dissection, – media
- intramural hematoma, –
- penetrating atherosclerotic ulcer originates in the intima
- New Classification
-
based upon the primary location of the lesion within the aortic wall:
-
aortic dissection involves the aortic media, penetrating aortic ulcer originates within the aortic intima,
-
aortic aneurysm is a disease of all three layers.
-
-
-
Intramural hematoma may be seen in any of the three fundamental pathologies.
- high risk of aortic rupture and sudden death
Pathogenesis
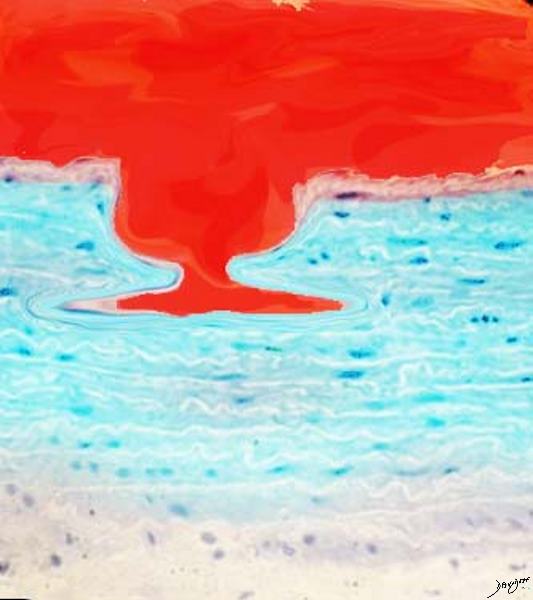
Ulcerated Plaque
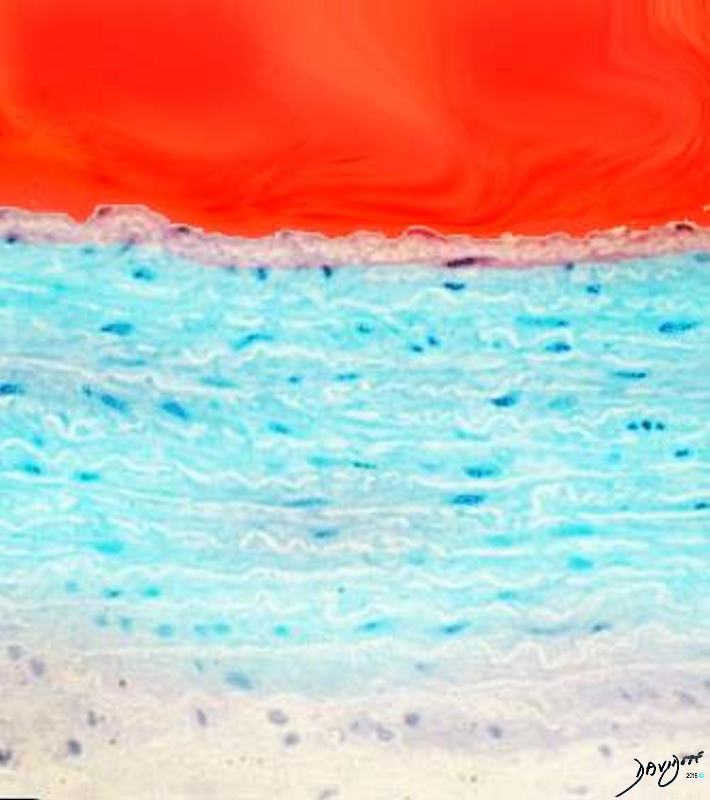
The lumen of the aorta with blood is demonstrated in red. The intima of the wall is the thin light pink layer just under the red luminal layer. The media or elastic layer is in teal, while the outer layer is a light yellow color
This diagram in a illustrates the normal aortic wall
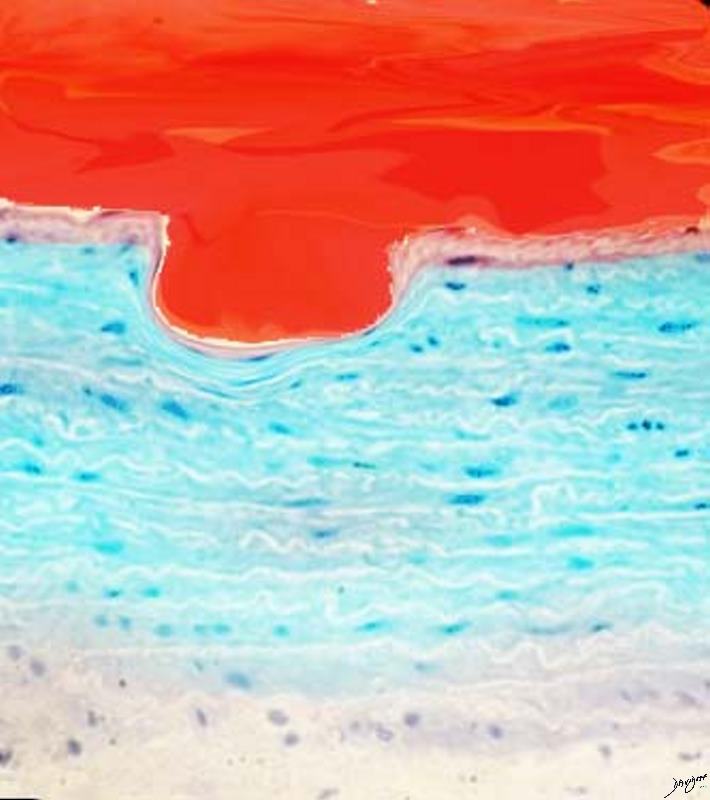
Image b shows the development of a cholesterol plaque commonly associated with acute aortic syndrome.
Courtesy Ashley Davidoff MD
TheCommonVein.net
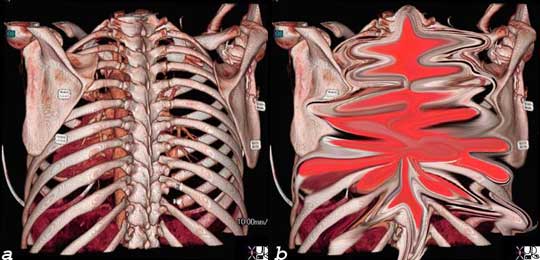
Usually Caused by Stretching of the Aortic Wall often as a result of a intramural hematoma
Ashley Davidoff
TheCommonVein.net

The pain is caused by distension of the aortic wall
Ashley Davidoff
TheCommonVein.net
Atherosclerosis Pathogenesis
Ulcerated Plaque
Clinical Presentation
Excruciating chest pain is the hallmark of the disease caused by acute distension of the aortic wall
Cause is distension of the aortic wall caused either by the acute intramural hematoma or by advancing penetrating ulcer or by the focal dissection
Pathogenesis of Atherosclerosis
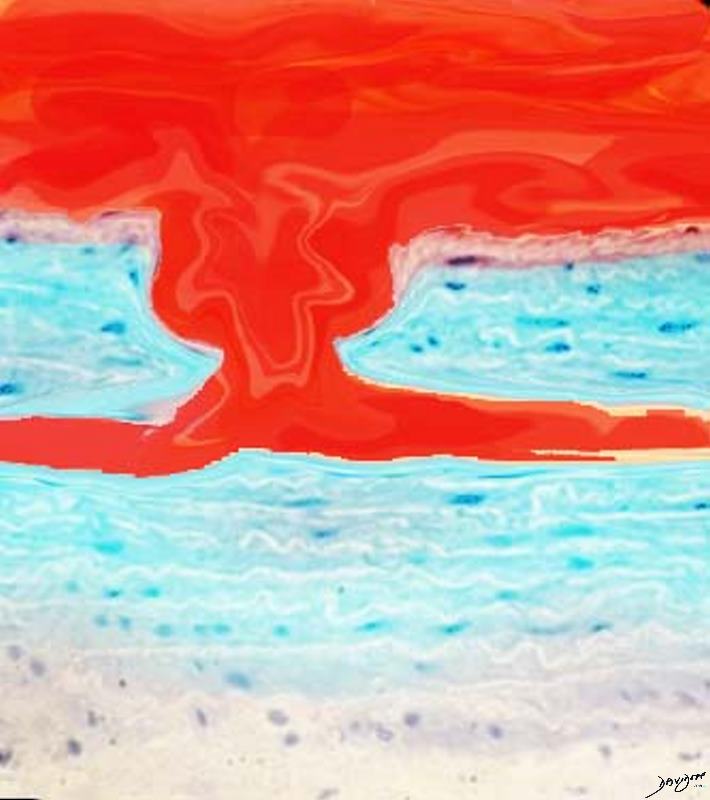
Starts out as a fibrofatty atheromatous plaque – –
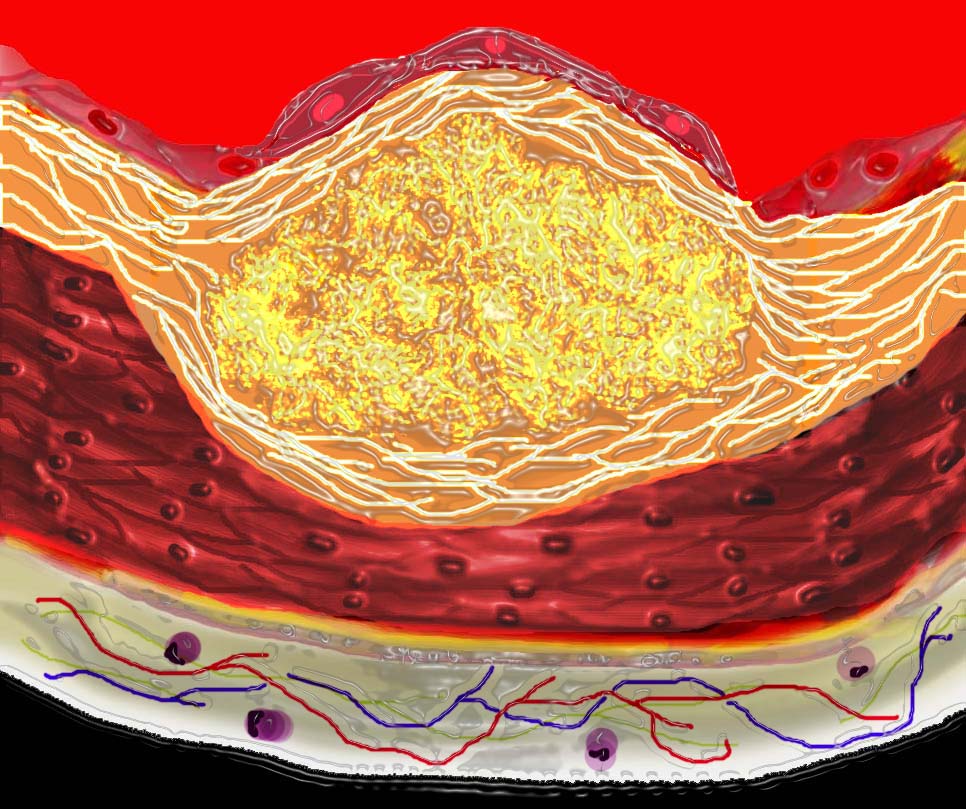
The diagram shows the atherosclerotic lesion in the subepithelial layer of the intima which is bulging both toward the media and toward the lumen. There is a central core of fat and necrotic debris, surrounded by fibrous elements which give the plaque its hardness to the feel. The accumulation of fibrous tissue heralds an advanced atherosclerotic lesion. 33801b01
Courtesy Ashley Davidoff MD. code heart artery atherosclerosis Davidoff art
Ashley Davidoff MD
THECOMMONVEIN.net
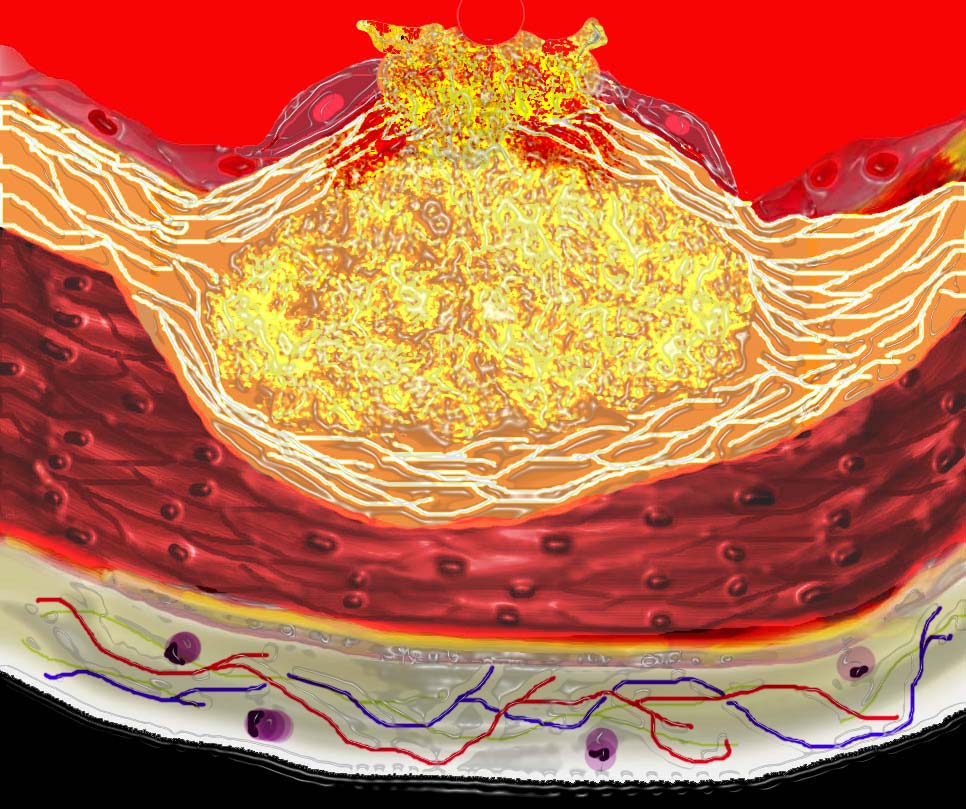
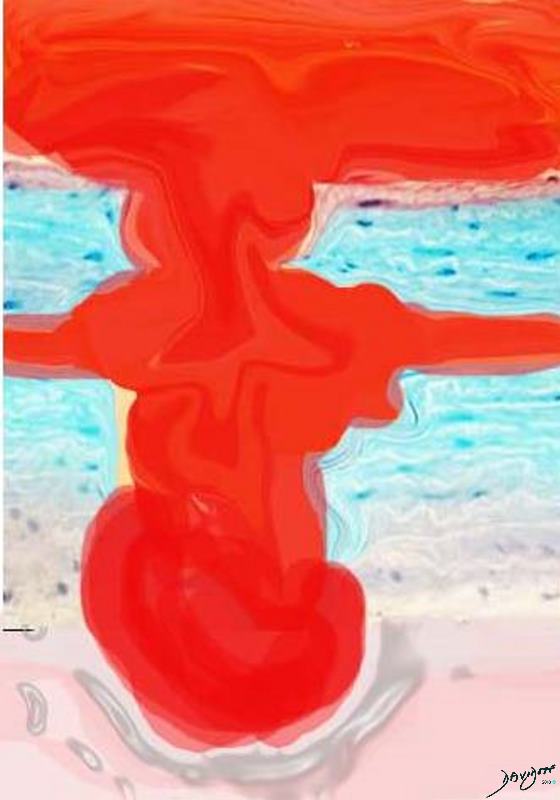
This diagram shows denudation of the endothelial layer with exposure and rupture of the contents of the atherosclerotic plaque in volcanic fashion into the lumen. This event is catastrophic and can result in acute thrombosis and may even be a fatal event. 33801d01 Courtesy Ashley Davidoff MD. code heart artery atherosclerosis atheroma vulnerable plaque drawing Davidoff art
Ashley Davidoff MD
THECOMMONVEIN.net
The pain simulates the pain of acute aortic dissection. Hence the same dramatic pain characteristics that occur in dissection apply to acute aortic syndrome, characterized by a sudden acute, severe, shearing or lancinating, pain that reaches maximum intensity at onset.
Similarly though as well, the symptoms may be minimal or absent.
Comparison to Dissection
The clinical features and pathology of the two entities can be quite different. Whereas dissection is usually in a younger age group, acute aortic syndrome is seen in the older atherosclerotic age group and is more commonly associated with hypertension.

Ashley Davidoff
TheCommonVein.net
Classic aortic dissection is characterized by the presence of intimal tear that usually progresses to the media and then rapidly dissects for quite a distance (sometimes the entire aorta) and will usually have a reentrance site.

This pathological specimen shows an aortic dissection starting at the root of the aorta and extending across the arch and into the descending portion. The false lumen is filled with clotted blood.
Courtesy of: Henri Cuenoud, M.D.
Intramural hematoma is characterized by the presence of severe atherosclerotic plaque, with acute hemorrhage into the aortic media which may remain as a hematoma in the media or may progress to a dissection. The dissection though is usually limited because the atherosclerosis and inflammatory changes and fibrosis present in the wall prevent s an easy route for progression. The reentrance of the dissection in AAS is usually absent and hence thrombosis of the focal dissection results.
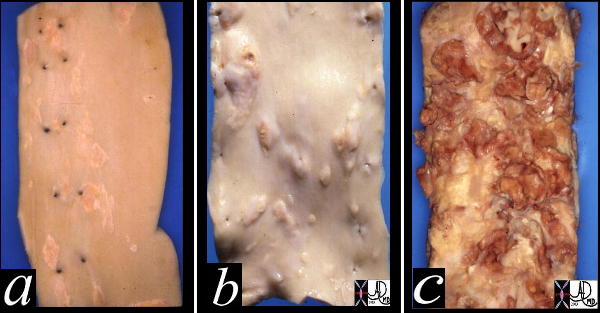
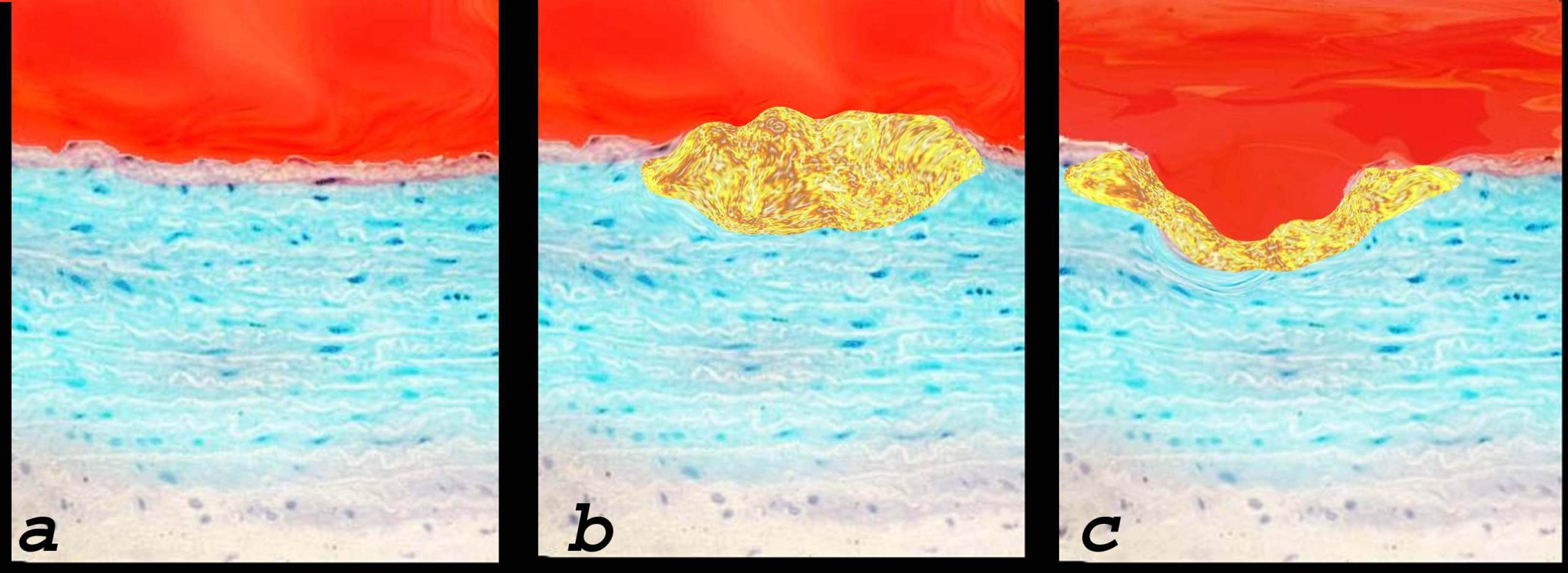
This image shows three pathological specimens of the aorta. In the first image minimally raised fatty streaks are noted. (a). In image b, the fibrous capsule causes raised fibrofatty nodules, while in c, there gas been rupture of the plaques, with friable atheromatous plaques abound. Courtesy Henri Cuenoid MD 13420c CVS artery aorta atheroscleosis atheroma fatty streaks fibro
THECOMMONVEIN.net
Please see page on Atherosclerosis of the Aorta
The diagram shows the atherosclerotic lesion in the subepithelial layer of the intima which is bulging both toward the media and toward the lumen. There is a central core of fat and necrotic debris, surrounded by fibrous elements which give the plaque its hardness to the feel. The accumulation of fibrous tissue heralds an advanced atherosclerotic lesion. 33801b01
Courtesy Ashley Davidoff MD. code heart artery atherosclerosis Davidoff art
Ashley Davidoff MD
THECOMMONVEIN.net
This diagram shows denudation of the endothelial layer with exposure and rupture of the contents of the atherosclerotic plaque in volcanic fashion into the lumen. This event is catastrophic and can result in acute thrombosis and may even be a fatal event. 33801d01 Courtesy Ashley Davidoff MD. code heart artery atherosclerosis atheroma vulnerable plaque drawing Davidoff art
Ashley Davidoff MD
THECOMMONVEIN.net
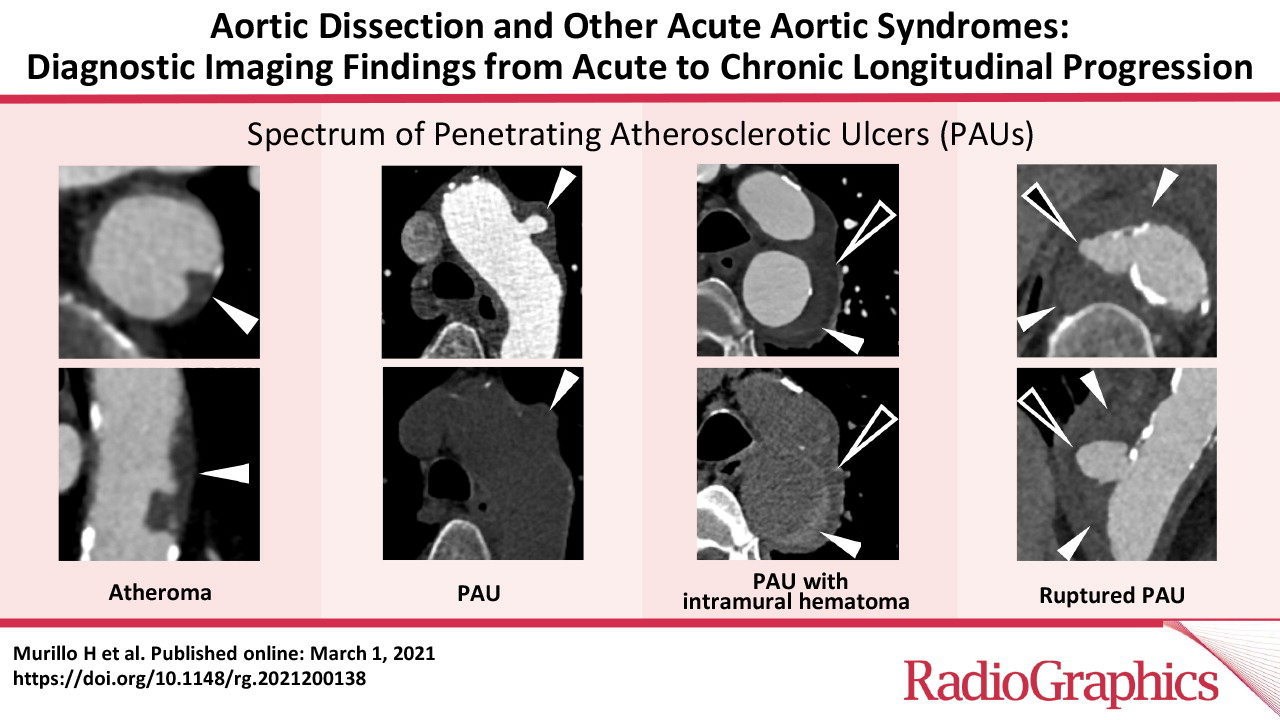
Murillo H et al Aortic Dissection and other Acute Aortic Syndromes Radiographics 2021
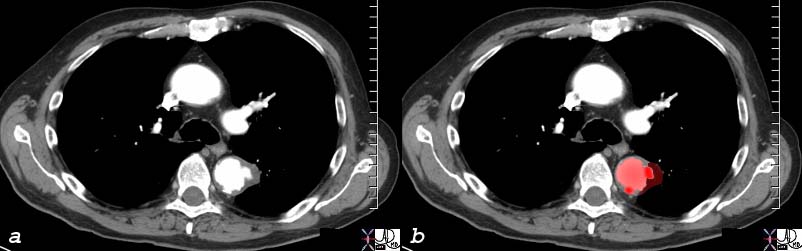
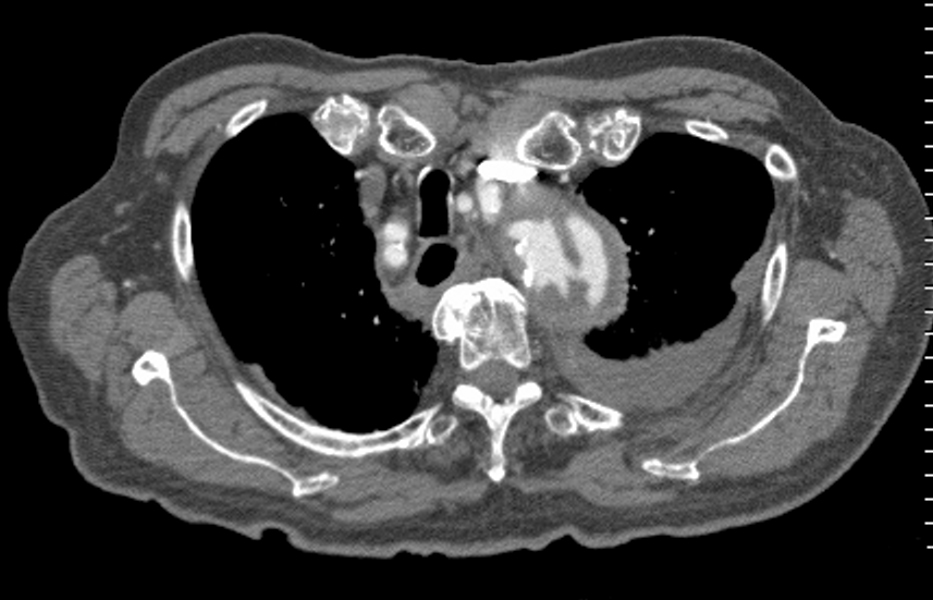
Penetrating ulcer in the descending descending thoracic aorta key words fx aortic ulcer fx atherosclerosis atheroma fx penetrating ulcer
acute aortic syndrome CTscan
48363
Courtesy Ashley Davidoff MD
The cause of AAS is an acute mural hematoma. This may result from a hematoma into a plaque, into a penetrating ulcer, or a hematoma in a focal dissection. The space occupation and sudden distension associated with the disease process by one of these disorders results in the classical pain syndrome. The disorders are best diagnosed by using a combination of non-contrast CT combined with a contrast enhancing CT.
The hematoma in the wall may be complicated by a classicial dissection , where the tear in the wall extends along the longitudianl plain. Aortic rupture can occur as well.
Treatment is based on the size position and nature of the lesion, as well as comorbid conditions, and thus would be either surgical or medical.
The pain is very similar to that of acute aortic dissection in that it is acute, severe, shearing or lancinating, but the clinical features and pathology of dissection is different. Whereas dissection is usually in a younger age group acute aortic syndrome is in the older atherosclerotic age group and is more commonly associated with hypertension. Classic aortic dissection is characterized by the presence of intimal tear that usually progresses to the media and then rapidly dissects for quite a distance (sometimes the entire aorta) and will usually have a reentrance site. Intramural hematoma is characterized by the presence of severe atherosclerotic plaque, with acute hemorrhage into the aortic media which may remain as a hematoma in the media or may progress to a dissection, but the dissection usually is limited because the atherosclerosis and inflammatory changes and fibrosis in general prevents easy route for progression. The reentrance of the dissection is usually absent and hence the focal dissection usually thrombosis.
Intact Intima
Ashley Davidoff
TheCommonVein.net
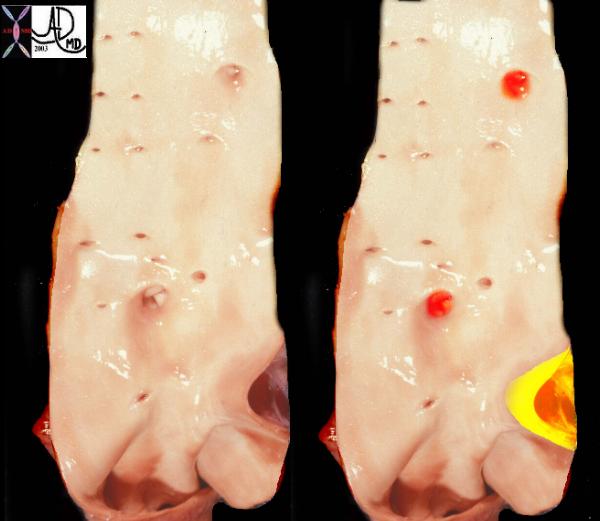
This is a post mortem specimen of the aorta of a patient with pulmonary atresia and bronchial collaterals. Overlaid in red are the enlarged orifices of the origins of the bronchial arteries. In yellow is the entrance of the PDA (patent ductus arteriosus) to the aorta Note in addition the normal appearing shiny appearance of the neonatal intima. Courtesy Ashley Davidoff MD 32628c a79-8
THECOMMONVEIN.net
18485c01 aorta artery hepatic artery renal artery splenic artery superior mesenteric artery SMA kidney severe atheroscleroris atheroma occluded renal artery spleen liver normal anatomy angiogram angiography
Ashley Davidoff MD
THECOMMONVEIN.net
Ashley Davidoff
TheCommonVein.net
Ashley Davidoff
TheCommonVein.net
Ashley Davidoff
TheCommonVein.net

Penetrating Ulcer |
| 48363 descending thoracic aorta fx aortic ulcer fx atherosclerosis atheroma fx penetrating ulcer CTscan Courtesy Ashley Davidoff MD |
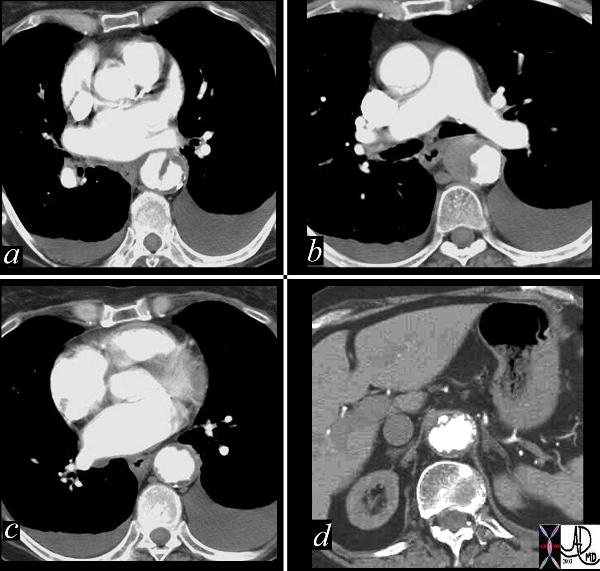
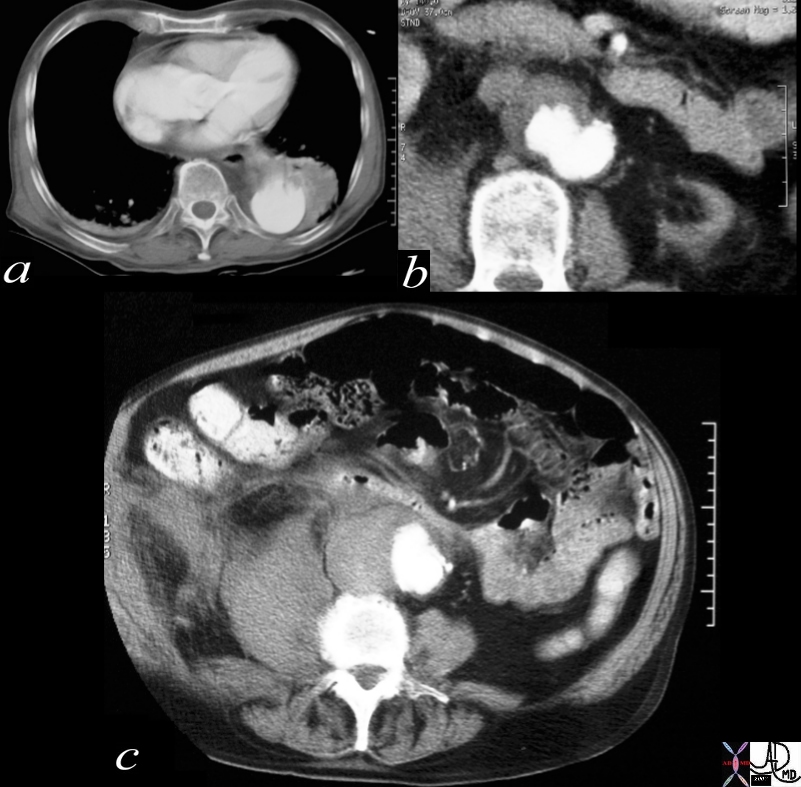
Penetrating Ulcer Mural Hematoma and Focal Dissection |
| This combination of images reflects the CTscan of a patient who presented with acute chest pain, and has findings reflecting a focal dissection of an atheromatous aorta. Note in (a) how thick the “intimal” flap is. Note also the mural dissection or hematoma with no flow within it. (b) Other parts of the descending aorta (c) and abdominal aorta (d) show only severe atheromatous disease. Courtesy Ashley Davidoff MD. 19416c code CVS aorta abdomen thorax dissection focal atherosclerosis |
Focal Dissection
A small focal dissection with flowing blood is seen, and this can either thrombose or progress to a full dissection
Ashley Davidoff
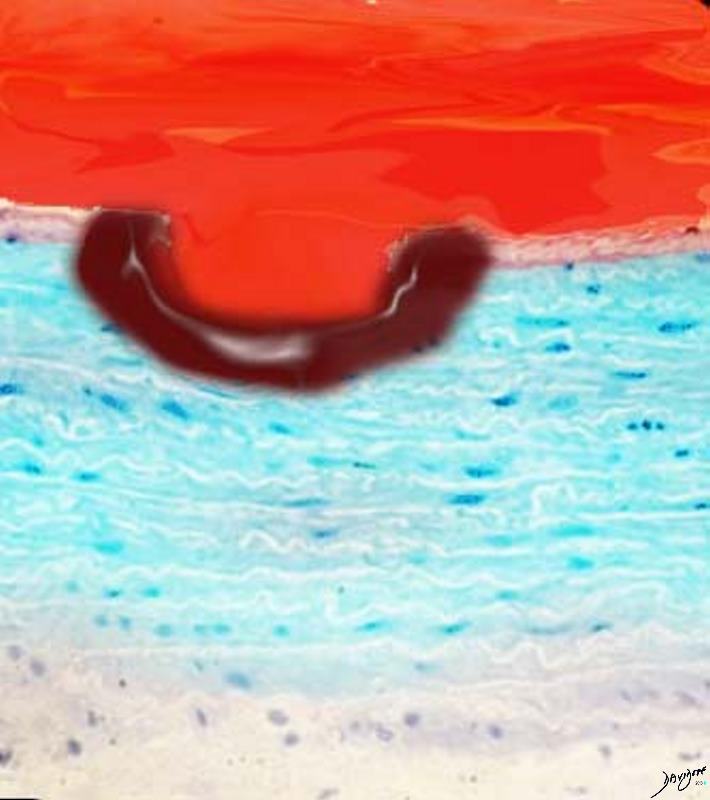
Progressive dissection with flowing blood is seen, and this can either thrombose or progress to a full dissection
Ashley Davidoff
TheCommonVein.net
Ashley Davidoff
TheCommonVein.net
Ashley Davidoff
TheCommonVein.net
Ashley Davidoff
The Common Vein
Ashley Davidoff TheCommonVein.net
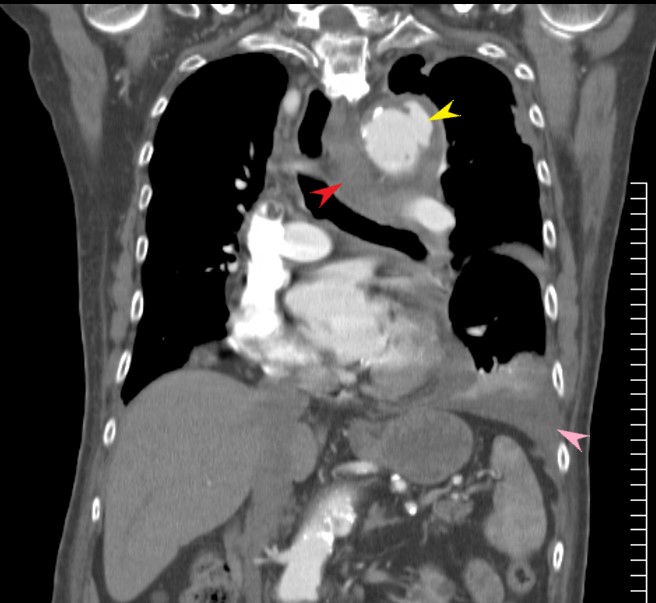
Penetrating Ulcer with Rupture |
| 17529c01 artery descending thoracic aorta abdominal aorta dx rupture pseudoaneumysm ulcerating plaque mural hematoma ruptured through aortic wall hemorrhage hematoma retroperitoneum CTscan Courtesy Ashley DAvidoff MD Ashley Davidoff MD |
|
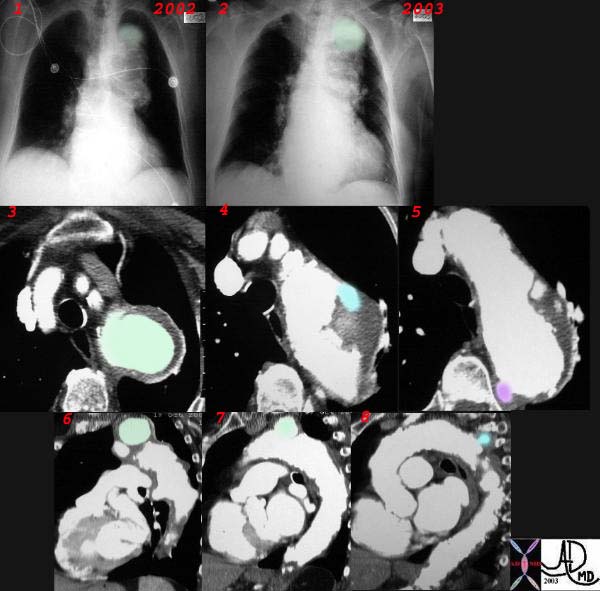
Penetrating Ulcer |
| This combination CXR and CT reveals an expanding aneurysm of the arch fromm 2002 to 3003. The CT shows three aneurysm in the arch of the aorta. The largest (green)seen in image 3,6, and 7 accounts for the finding in the left apex of the CXR, while a second pseudoaneurysm is seen on the lateral border of the knob (blue – 4,8) and a penetrating ulcer medially (purple 5) 32029c2 |
Links and References
Murillo H et al Aortic Dissection and other Acute Aortic Syndromes Radiographics 2021
Grist T and Rubin G from Diseases of the Chest Breast and Heart Chapter 18 Imaging Acute Aortic Syndromes